THIS WEBSITE USES COOKIES
We use cookies to personalise content, to provide social media features, and to analyse our traffic. By choosing 'allow all cookies', you consent to our cookies.
To find out more, read our privacy policy and cookie policy.
The ICLEAR intervention is a novel, staged, multi-faceted approach to care for those with advanced COPD to identify and respond to their end-of-life care needs. The rationale of ICLEAR is to identify palliative care needs and facilitate discussions with patients, families and all care providers to prepare an action plan for agreed future care strategies and to integrate palliative care into present and future care strategies. ICLEAR-EU is a person-centred and family-centred non-pharmacological service intervention in which respiratory teams in the hospital collaborate with interdisciplinary palliative care teams and with primary care to promote shared decision-making and advance care planning, improve symptom treatment and comfort care, and prevent rehospitalisation after an exacerbation. ICLEAR-EU is based on an existing intervention developed and pilot tested in the UK.
The ICLEAR-EU intervention aims to provide clear, easy-to-read and evidence-based broad, multimodal clinical guidance to healthcare professionals to shift the paradigm towards identifying the goals of care, optimising personalisation of care based on patient priorities and preferences and enhancing overall integration of care by improving communication within the clinical team and across healthcare sectors (respiratory, primary and palliative care services). The ICLEAR-EU intervention is an evidence-based approach that emphasises communication and collaboration between patients, family caregivers and healthcare professionals. The ICLEAR intervention has five core components and two implementation strategies.
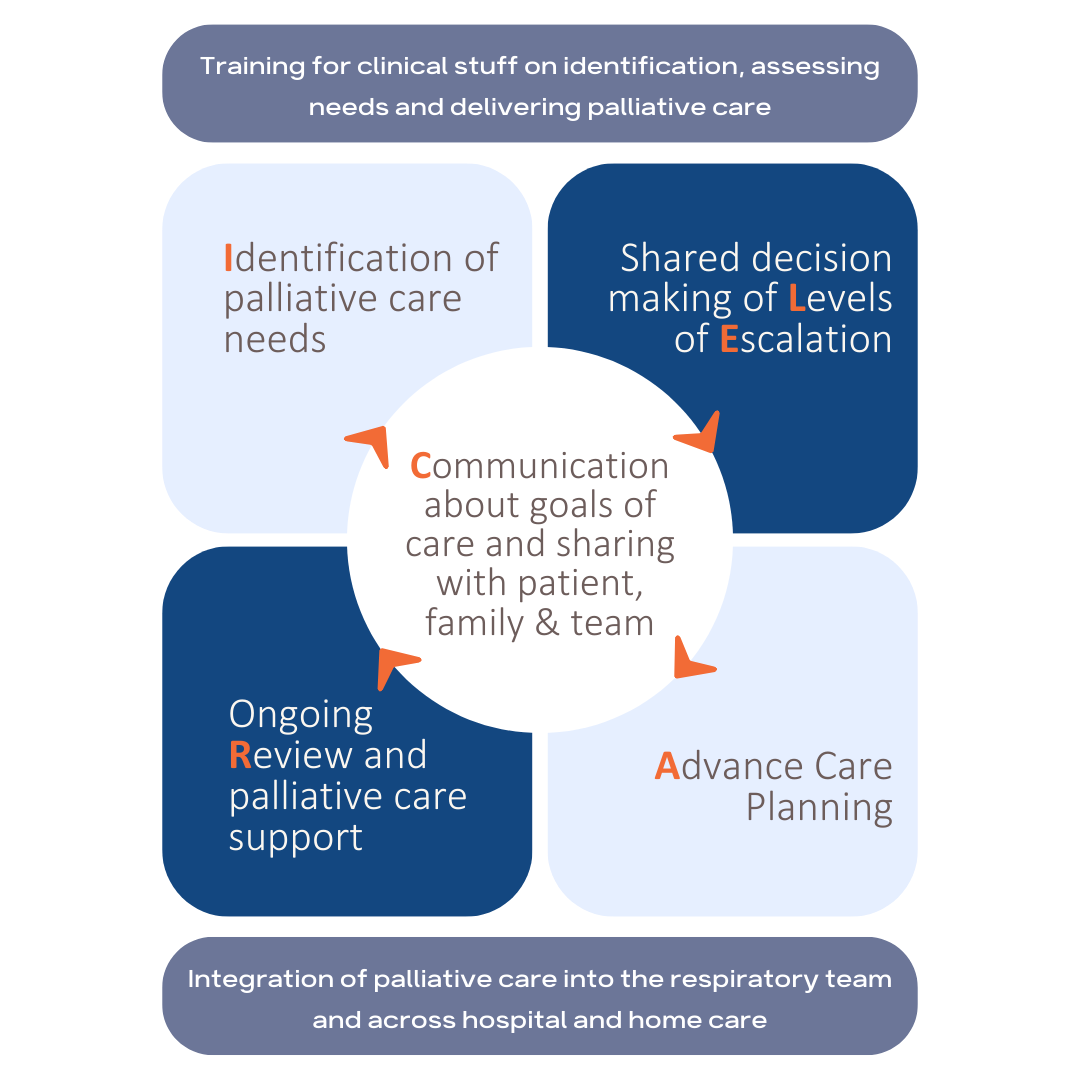
Identifying the risk of deterioration and mortality in COPD is important so that people can be offered appropriate and timely interventions. Multidisciplinary meeting is held to apply the ICLEAR tool to determine palliative care needs.
This improves coordination of care, promotes agreed future care strategies and has an impact on illness understanding and future disease management. Communication and interaction are present throughout the care trajectory: between disciplines, between health professionals and patient + family.
This promotes agreed future care strategies and has an impact on illness understanding and future disease management. Once palliative care needs are determined, the multidisciplinary meeting discusses the care options and creates a patient management plan.
Advanced care planning (ACP) can assist patients in articulating goals of care and their preferred place of death. The ACP conversation is linked to the care plan for future exacerbations. ACP is initiated with patient and family carer (if present) by a member of the respiratory team or the palliative care team.
Continuity of care and support allows patients to be cared for in their preferred place. Follow-up visits are conducted by health professionals. The patient management plan is reviewed in future live or telephone consultations.